

Rotator Cuff Tears: What They Really Mean
(and When You Actually Need Surgery)
You've been dealing with shoulder pain for a few weeks. Your GP refers you for an MRI. The results come back, and there it is — "rotator cuff tear." Suddenly, the conversation shifts from "maybe it'll settle down" to "we should talk about surgery."
It's a scenario we see regularly at Richmond Rehab. But here's the thing, a rotator cuff tear on a scan and a rotator cuff tear that needs surgery are not necessarily the same thing. Not by a long shot.
What Is the Rotator Cuff?
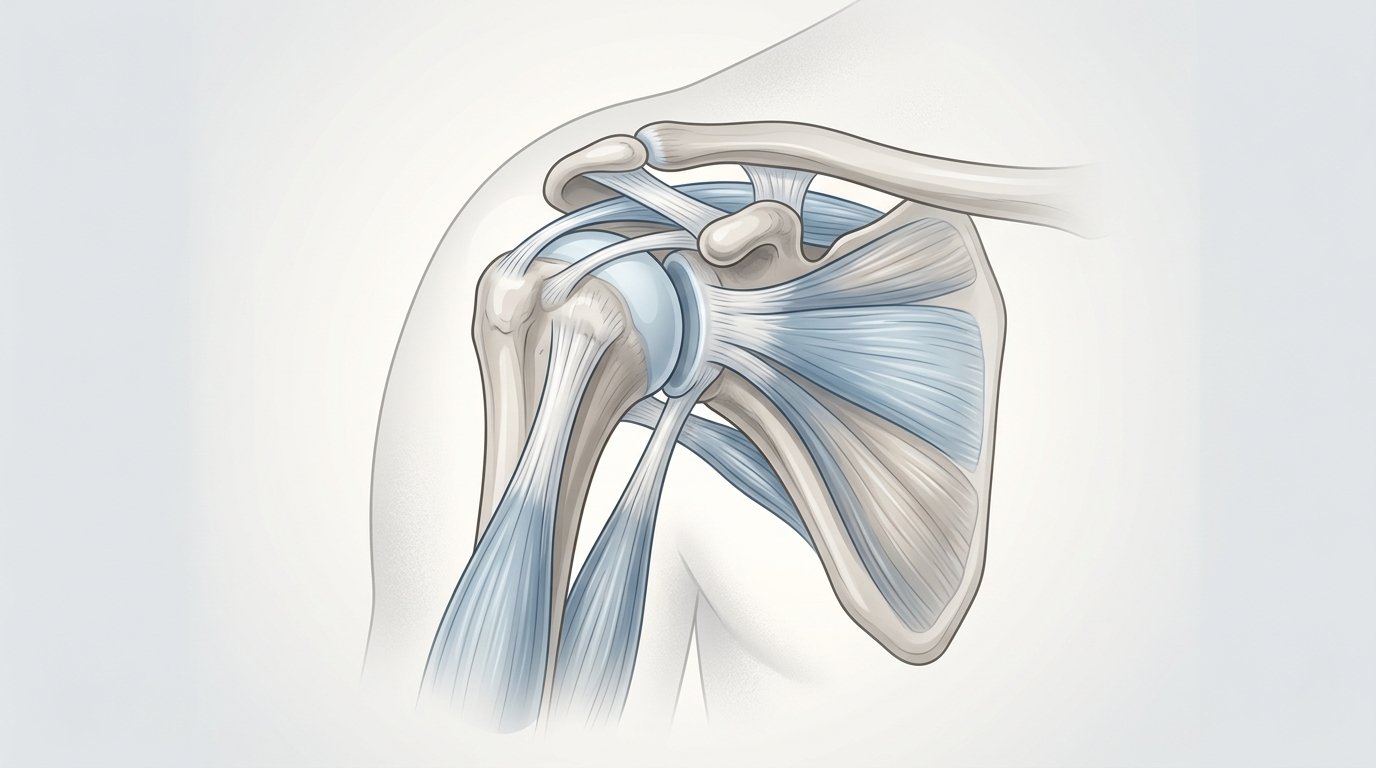
The rotator cuff is a group of four muscles; supraspinatus, infraspinatus, teres minor, and subscapularis. These wrap around the shoulder joint and keep the ball of the humerus properly seated in the socket. They're the fine-tuners of shoulder movement, coordinating stability and control for everything from reaching overhead to throwing a ball.
A "tear" means one or more of these tendons has a partial or full-thickness disruption, which range from minor fraying to a complete rupture. The size, location, and cause of the tear matter enormously when it comes to deciding what to do about it.
How Common Are Rotator Cuff Tears, Really?
More common than most people realise. Yamamoto et al. (2010) conducted ultrasound screening across a general population of 683 people and found rotator cuff tears in 20.7% of all shoulders examined. Milgrom et al. (1995) found a similar picture, with tear prevalence rising sharply with age, present in roughly 54% of people over 60.
Here's the part worth sitting with: many of these people had no shoulder pain whatsoever.
A significant proportion of rotator cuff tears in the general population are completely asymptomatic. The shoulder is functioning, the person is active, and the tear is just... there. So when a scan picks one up, we need to be careful about how much weight we give the report on its own.
Does a Tear Always Progress?
Not always — but it can. Moosmayer et al. (2013) followed 50 people with asymptomatic full-thickness tears over three years. 36% developed symptoms during that period. The other 64% remained pain-free. Those who became symptomatic (pain or weakness) tended to have larger tear progression (an average increase of 10.6mm versus 3.3mm in the stable group) and greater muscle deterioration.
So some tears do progress and cause problems. But the majority in that study didn't. And the scan alone can't tell you which group you'll fall into — which is exactly why a clinical assessment gives you so much more than an imaging report ever can.
So When Does Surgery Actually Make Sense?
Surgery is not the wrong answer — for some presentations, it's clearly the right one. Acute, traumatic tears, particularly in younger or more active patients, often benefit from early surgical repair. Large complete tears with significant muscle involvement may also be good surgical candidates, especially if a structured conservative programme hasn't moved the needle.
What the evidence challenges is the assumption that surgery is automatically better than physiotherapy for the typical degenerative rotator cuff tear.
Longo et al. (2021) reviewed & analysed 6 studies, comparing surgery with conservative management for rotator cuff tears. Functional outcomes at two years were comparable between groups. Surgery showed a modest advantage in pain reduction at 12 months, but longer-term functional differences were not statistically significant.
Heerspink et al. (2015) found similar results in their study which directly comparing surgical repair with physiotherapy-led conservative care for degenerative tears.
Again, no significant difference in shoulder function at two-year follow-up.
That's not an argument against surgery. It's an argument for asking the right question before you book in for it.
What Can Physiotherapy Do?

Quite a lot. A well-structured rehabilitation programme targeting rotator cuff strength, scapular control, and movement mechanics can restore function, reduce pain, and help people return to the things they want to do, often without ever going near a theatre.
The key distinction is that conservative management doesn't mean doing nothing and hoping for the best. It means working systematically through a progressive loading programme, guided by someone who understands shoulder biomechanics and knows when the clinical picture warrants a surgical referral.
Where to From Here?
If you've received a diagnosis of a rotator cuff tear, whether you're in significant pain or just managing, the most useful next step is a proper clinical assessment. Not another scan, and not an immediate surgical consult. A thorough shoulder assessment maps your pain, your function, your goals, and the nature of the tear into a picture that an MRI report simply can't provide on its own.

At Richmond Rehab, Jesse Dean is our go-to guy with shoulder complaints. He has a particular interest in shoulder injuries and post-surgical shoulder rehabilitation.
If you're sitting on an MRI result with more questions than answers, he's a good place to start.
References
Heerspink, F. O. L., van Raay, J. J. A. M., Koorevaar, R. C. T., van Eerden, P. J. M., Westerbeek, R. E., van't Riet, E., van den Akker-Scheek, I., & Diercks, R. L. (2015). Comparing surgical repair with conservative treatment for degenerative rotator cuff tears: a randomized controlled trial. Journal of Shoulder and Elbow Surgery, 24(8), 1274–1281. https://doi.org/10.1016/j.jse.2015.05.040
Longo, U. G., Risi Ambrogioni, L., Candela, V., Berton, A., Carnevale, A., Schena, E., & Denaro, V. (2021). Conservative versus surgical management for patients with rotator cuff tears: a systematic review and meta-analysis. BMC Musculoskeletal Disorders, 22(1), 50. https://doi.org/10.1186/s12891-020-03872-4
Milgrom, C., Schaffler, M., Gilbert, S., & van Holsbeeck, M. (1995). Rotator-cuff changes in asymptomatic adults: the effect of age, hand dominance and gender. Journal of Bone and Joint Surgery (British), 77(2), 296–298. https://doi.org/10.1302/0301-620x.77b2.7706351
Moosmayer, S., Tariq, R., Stiris, M., & Smith, H.-J. (2013). The natural history of asymptomatic rotator cuff tears: a three-year follow-up of fifty cases. Journal of Bone and Joint Surgery (American), 95(14), 1249–1255. https://doi.org/10.2106/JBJS.L.00185
Yamamoto, A., Takagishi, K., Osawa, T., Yanagawa, T., Nakajima, D., Shitara, H., & Kobayashi, T. (2010). Prevalence and risk factors of a rotator cuff tear in the general population. Journal of Shoulder and Elbow Surgery, 19(1), 116–120. https://doi.org/10.1016/j.jse.2009.04.006